It was a crisp autumn morning when Darren came to my gastroenterology clinic, dressed in a suit and a tie. A university professor with two PhDs, he had been lecturing students that morning on the valence electrons within atoms.
Clearly, he was a man at ease with his intellect. Physically, though, he was not. For years, he’d felt sluggish and bloated – and his bowel movements were sporadic at best.
When I asked him what his last poo looked like, he was mortified. ‘I don’t look at my poo. What’s it supposed to look like?’ Over the next few months, I saw the same pattern on repeat in my newly opened clinic in Massachusetts General Hospital.
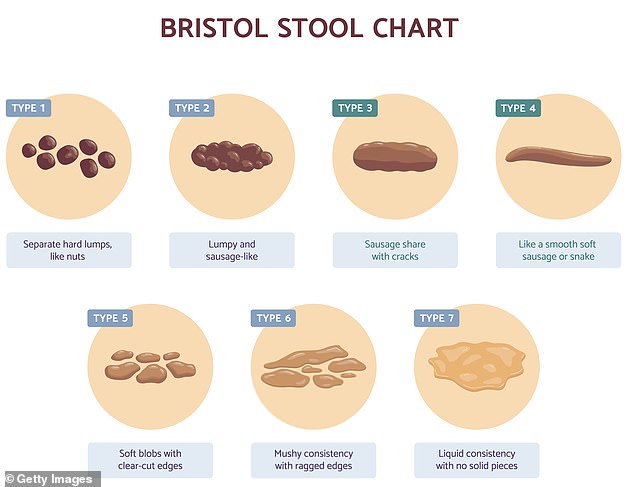
Accomplished athletes, computer scientists and media high flyers – people you might expect to be more informed – came seeking my advice on the very basics about their bowels. What colour poo was normal? Should they worry if it wasn’t a smooth sausage shape? And how often should they be going?
They also wondered about subtler matters, too. What kind of fibre was best to eat? Were ultra-processed foods harming their bowel health? What daily activities help guts function smoothly? As a gastroenterologist and an assistant professor of medicine at Harvard Medical School, I have spent years researching the intricacies of gut health.
In 2024, I found that Parkinson’s disease could be predicted by gut problems decades before people developed tremors.
My team’s findings, published in the journal JAMA Network Open, concluded that having an old gastrointestinal injury, such as a stomach ulcer, was associated with a 76 per cent increased risk of later developing Parkinson’s. (We noted that stomach ulcers, as well as being aggravated by stress, are prevented by dopamine, the very chemical that is depleted in the brains of people with Parkinson’s.)
Despite all the recent well-publicised scientific advances we have made in understanding gut health, I am still often surprised to find my patients lack basic knowledge about what’s normal when it comes to bowel function, writes Dr Trisha Pasricha
Today I am also director of the Institute for Gut-Brain Research at Beth Israel Deaconess Medical Center in Boston, leading a research laboratory at the forefront of gut-brain science.
Despite all the recent well-publicised scientific advances we have made in understanding gut health, I am still often surprised to find my patients lack basic knowledge about what’s normal when it comes to bowel function, and have a general embarrassment around it.
Yet none of this is something to be ashamed of – indeed, knowing about such things provides valuable insight into the state of your overall health and is vital to a happy, healthy life.
Through treating thousands of patients, I’ve discovered that there are a few simple tips that can help fix the bloating, constipation, diarrhoea, haemorrhoids and cramps that blight so many lives.
These aren’t just issues which affect older people, either. Many of my patients are in their 20s and 30s. And a recent study of more than 5,000 people in the US, Canada and the UK found 34 per cent of those aged 18 to 34 experienced at least one bowel disorder (e.g. chronic constipation or diarrhoea) – in contrast to 22 per cent of those over 65.
Let’s take the first two most common questions: colour and frequency.
Poo normally should be a chocolate brown: bile – a digestive fluid produced by the liver – is a yellowish brown to dark green, and when mixed with our gut bacteria, it turns dark brown.
And the number of times we poo each day – or each week! – is variable. Decades of study have concluded that anywhere from three times per day to once every three days is within the healthy range.
In the UK between one and three times a day is normal – while in eastern India, the average is 14 stools per day (partly down to local diet, which is heavier in fibre and spice).
Here are some of my top tips for keeping you regular and content down there…
Never hold it in!
Often people will suggest drinking more water to make it easier to poo – and yes, hydration is important, but it’s not always the primary issue.
More significant is going as soon as you feel that urge. Never hold in a poo – the longer it sits in your colon, the more water will be drawn out of it, making it harder to go.
That’s because the colon believes its primary job is absorbing water – and it does so astonishingly well, absorbing up to five litres of fluid per day, meaning there’s only so much that drinking extra water can counteract this action.
The longer poo sits in your colon, the drier it becomes, making it harder to pass as it transforms into dense pebbles.
Don’t use your phone on the loo
Looking at your smartphone on the loo is a modern-day habit – but a study my team ran, published in the journal PLoS One last year, proved this is something you should never do, as it is associated with a significantly heightened risk of haemorrhoids.
We surveyed 125 people just before they underwent colonoscopies (where the colon is examined using a tiny camera), including questions on how often they pooed, how much fibre they regularly consumed, how long they spent on the loo, and what they did while there.

Using smartphones on the loo was associated with a 46 per cent increased risk of haemorrhoids in a study
We found 66 per cent of the participants used their smartphones while pooing. Both groups – phone using and non-phone using – suffered similar rates of constipation. But using smartphones on the loo was associated with a 46 per cent increased risk of haemorrhoids.
Why? Because it increased the time spent on the loo, thus placing unnecessary pressure on the anal area. Some 40 per cent of smartphone users spent more than five minutes on the loo to poo, compared with only 7 per cent of non-users.
I tell my patients not to spend any more than five minutes on the loo – set a timer if you have to. If you’re not done after that, give up and come back after a walk.
Cramp is normal
Before you poo, it’s normal to feel some cramping and urgency – this is your body’s internal mechanisms telling you it needs to push the faeces out. But those signals shouldn’t feel painful.
And pain while the poo is on its way out is also abnormal – it would make me worried about an issue near the anal sphincter, such as a haemorrhoid or fissure (a small tear in the anus, often caused by constipation).
Night-time loo visits are a worry
When we get to a certain age, night-time trips to urinate become more likely – especially for men who may have enlarged prostate glands (which can prevent the bladder emptying fully).
But pooing at night is a different story. That’s because medically speaking, it’s an activity that should only occur during the day – as this is when our colon is most active.
Indeed, one study from the 1990s at the University of Bristol on the bowel patterns of nearly 1,900 people found that the most common time of day to poo is between 7am and 9am, with a second peak after about 6pm (when people eat what is typically the largest meal of the day).
Pooing should not wake you up from sleep. When someone comes to me saying they often get up out of bed to poo at 3am – or worse, have accidents they only discover in the morning – I run tests to see what’s going on. It may indicate that you have inflammation in your bowel, for instance.
Wellness detoxes are pointless

Dr Trisha Pasricha has spent years researching the intricacies of gut health
So many people seem to believe that lurking in your colon are ‘toxins’, and the longer your poo stays in your intestines, the more dangerous these are. It’s this idea that has led to wellness detoxes, enemas and colon cleanses. But there is zero scientific basis for it.
Indeed our liver is our detox organ, not our colon.
Most of the components of our food (apart from fibre) are absorbed by the small intestine, then pass into a vein and directly to the liver.
And everything we have absorbed is then filtered and processed by our liver, including any unwanted substances, prior to passing into your main bloodstream.
You certainly don’t have pounds of poo sitting around for weeks inside your colon that only an intense juice cleanse can fix.
Barring any major motility disorder your doctor may have diagnosed (linked to damage to the nervous system, for instance), the poo you do have in your body is merely in transit – which for most people takes a couple of days.
Another reason to avoid UPFs
Ultra-processed foods (UPFs) have changed how we poo – and not for the better.
In a 2022 study, researchers assigned participants to eating the same diet for 11 days; the only difference was that one group’s meals contained carbomethylcellulose, a common synthetic emulsifier in many UPFs.
People whose meals included the emulsifier experienced increased abdominal discomfort after eating.
Another 2022 study found that people assigned to a diet containing common added sweeteners (e.g. aspartame, sucralose and saccharin) experienced new diarrhoea, constipation and pain after eating – symptoms that were all reduced for those assigned to diets with minimal sweeteners.
It’s very difficult, then, to have regular, predictable bowel movements and support gut health on an ultra-processed diet.
A morning poo is ideal
Very few people know of the internal mechanisms in your body that help you poo. But with a little guidance, you can maximise the potential of your loo visits.
The most important kind of colon contractions are called high-amplitude propagated contractions (HAPCs).
Unlike the background movement always churning in your gut, HAPCs happen only a few times per day and generate a strong force that propels poo into the rectum – the final segment of the colon.
While HAPCs can occur spontaneously, and certain medications – such as the popular laxative bisacodyl – help induce them, there are times when they are naturally more likely. (The gastrocolic response, see box, that’s triggered by coffee is one of the physiological reflexes that in turn could trigger an HAPC.)
This means if you time your loo visits, you can combine HAPCs with the other mechanism within your body that helps you poo: the Valsalva manoeuvre, the instinctive bearing down and straining we experience in a bowel movement – while breathing out against a closed mouth.
Straining can be hard. In fact, some people Valsalva so intensely they pass out with the effort – I’ve seen this among my hospitalised patients more than a few times.
So how can you combine the efforts of your Valsalva with a HAPC? Researchers have found that your colonic activity spikes threefold in the first hour after waking. But that increase in activity, including HAPCs, doesn’t last more than this. Gastroenterologists advise, then, that early morning is an ideal time to poo.
What colour your poo shouldn’t be
I’ve seen every colour poo – from blue to yellow to green. Normally, these are just determined by your diet. Fatty foods, for example, produce yellower poos as you produce more bile (which is yellow-ish green) to digest them: anyone on a keto diet – which is high in fat, low in carbohydrates – should watch out for this side-effect.
However, there are some colours that are concerning, and demand medical attention. An obvious one is red or black, which can indicate bleeding.
Patients who tell me they have white or clay-coloured poo also have my full attention: it means something is blocking bile from reaching the gut. The most common reason for this is a gallstone.
Silver poo – highly rare – is a medical emergency, as it is the result of a blocked bile duct and bleeding from your upper gastrointestinal tract. So the white poo, mixing with shiny black acidified blood, makes silver.
The power of kiwis

A trial found that patients with constipation who ate two green kiwis a day increased poo frequency
Fibre helps maintain healthy habits because it ensures we retain more water in our faeces as it passes through our system, making it easier to pass. But what kind of fibre is best?
In terms of supplements, I prefer psyllium, as it’s a soluble fibre that forms a gel in contact with water and most effectively retains it within the stool.
In dietary terms, though, I usually say just increase fibre consumption any way you can – but certain high-fibre foods have been particularly well studied for their effects: prunes and kiwis.
A 2021 trial found that patients with constipation who ate two green kiwis a day, 100g prunes a day, or 12g of psyllium per day for four weeks all equally increased poo frequency and decreased straining during a bowel movement. More people preferred kiwis, though, because they also improved their bloating.
Always use two-ply paper

In an ideal world, we should all use a bidet after pooing for improved hygiene and comfort. I also recommend bidets to any patient who struggles with balance or coordination reaching to wipe.
Sadly, though, bidets are rare in the UK. It’s important, then, to be careful with loo paper. This is because the anal area is highly sensitive – dense with nerve endings and is not meant to be scrubbed harshly. Never wipe or rub: Gently dab away any excess instead with the tissue to minimise irritating your skin or flaring up any angry haemorrhoids.
But dabbing doesn’t work so well if you have flimsy loo paper. I’d go so far as to say one-ply paper should be banned, and two-ply is the bare minimum. Thin loo paper is rougher on the skin, which can lead to damage to the anal area.
© Dr Trisha Pasricha 2026
Adapted from You’ve Been Pooping All Wrong by Dr Trisha Pasricha (Thorsons, £16.99) published on April 9. To order a copy for £15.29 (offer valid to 11/04/26; UK P&P free on orders over £25) go to mailshop.co.uk/books or call 020 3176 2937.